Syllabus: GS2/Health Issues
Context
- A new study found that the key health policy committees since Independence are neglecting diverse perspectives critical for public health systems.
About
- The centralisation of health policy in India refers to the process where the central government plays a significant role in the formulation and implementation of health policies.
- It is evident in various aspects of the health sector, including policy-making, funding, and regulation.
- However, a new study found key health policy committees since Independence are overrepresented by men, doctors, bureaucrats and individuals from New Delhi — neglecting diverse perspectives critical for public health systems.
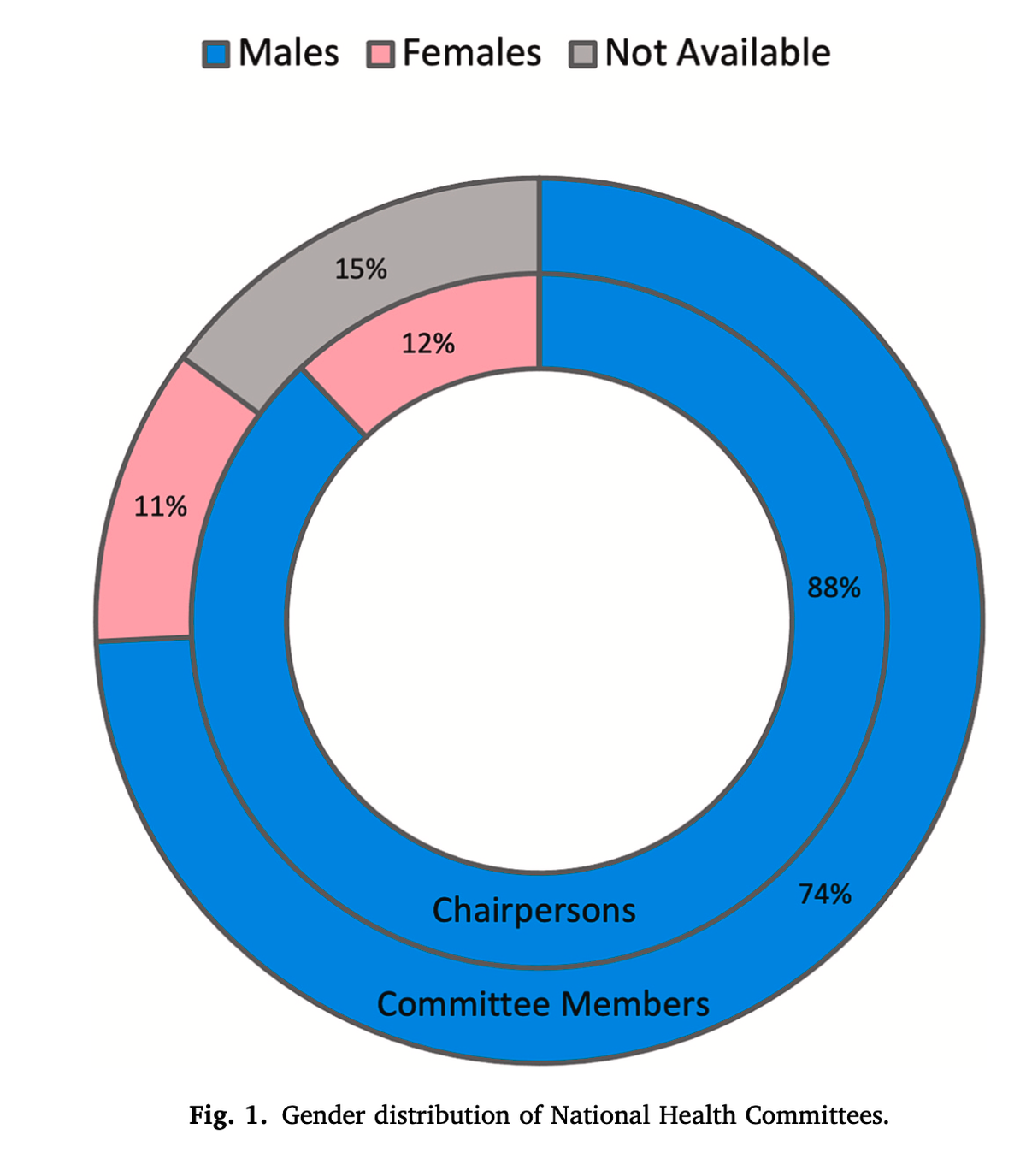
- For Instance: women constitute almost half of all of India’s health workers. Yet, only a small chunk of them reach the leadership and decision making positions.
Related Concerns
Diversity Gaps:
- Lack of Diversity in Health Committees: According to an analysis of India’s National Health Committees between 1943 and 2020, the Health Committees are facing a problem of ‘over-concentration’ of not just men, but of doctors, individuals from Delhi-NCR, and bureaucrats.
- The lack of diversity and representation in India’s health committees and leadership positions is hindering equitable health policies and outcomes.
- Low Participation of Women: Official data suggests women constitute almost half of all of India’s health workers.
- However, about 18% of the women make it to the top of the pyramid, reaching leadership positions across health panels, committees, hospitals, colleges and ministries.
- Only 11% of women were present in 23 health committees, and there was no woman present in 36% of the committees.
- For instance, the Devi Shetty Committee was formed for the Prevention and Management of COVID-19 Third Wave in 2021.
- The committee was primarily led by male clinicians, lacking the diverse expertise needed to tackle a global health crisis.
- Initially comprising only men, the committee added two women after facing criticism.
- Women make up 29% of doctors, 80% of the nursing staff, and nearly 100% of Accredited Social Health Activists (ASHAs) in the country.
- Moreover, their job is classified as ‘care work’, not technical enough, further devaluing their knowledge. Women across the workforce, on average, earn 34% less than men.
| Do you know? – 70% of CEOs and board chairs across 201 global health organisations were men, and just 5% of leaders were women from low and middle income countries. – A report from Women in Global Health found women occupy only 25% of senior positions and 5% of leadership roles in the healthcare sector, despite making up 70% of the overall global health workforce. |
Regional Disparity:
- Medical leadership is concentrated in Delhi-NCR (with almost half of the members present there), and there is a high degree of influence from doctors and government officials.
- However, post-2000, Health committees are getting more diverse, including women, NGOs and non-medical academia.
- At the same time, centralisation has increased, from 53% before 2000 to 83% in recent years.
- Neglecting Preventive Care: A tendency to view public health as the clinical medicine in India. It’s more of a disease cure, not about dignity and care.
- The ‘neglect of preventive care’ reflects in how nurses are treated, how ASHAs are paid, and how medical doctors are over-represented in these health committees.
- A ‘Top-down Approach’: India’s National Health Policy, read in tandem with NITI Aayog’s ‘Vision 2035’ white paper on public health surveillance, promotes diversity in political, policy, technical, and managerial leadership at both national and state levels.
- However, a Lancet paper noted that there is a ‘larger leadership competency gap’ in Indian health policy, which has many dimensions, and gender is a part of it.
- Inadequate Funding for Urban Health: The condition of the National Urban Health Mission (NUHM) remains pathetic due to inadequate funding1. This has resulted in major shortages of public health services during the COVID-19 pandemic, particularly for urban Indians.
- Challenges in Reaching Marginalised Communities: There are considerable challenges in reaching the poor and marginalised communities in urban areas and ensuring equitable health outcomes.
- The policy focus so far has been mostly in rural and tribal areas on improving access to health services and strengthening the health systems.
- Maternal and Child Health: Though India has made substantial improvements in reducing maternal and child mortality over the decades, much more remains to be done in terms of bringing more people into institutional systems, reducing anaemia, and addressing inequity in healthcare.
| Health and Constitution of India Constitutional Provisions: – Public Health and Sanitation, Hospitals, and Dispensaries fall under the State List (List II, Schedule VII). – Family Welfare and Population Control, Medical Education, Prevention of Food Adulteration, and Quality Control in the Manufacture of Drugs are included in the Concurrent List (List III, Schedule VII). – The Central Council of Health and Family Welfare (set up under Article 263 of the Constitution) enables consideration and recommendation of broad lines of policy in regard to matters concerning health and family welfare. Right to Health: – While the Constitution of India does not explicitly mention the right to health, it has been interpreted by the judiciary to be an integral part of the right to life under Article 21. |
Conclusion and Way Forward
- According to the Women in Global Health Report, hiring, promotion and rotating doctors decisions should be made taking into account identity-based challenges; efficient, anonymous systems to report misconduct; adapting systems to “encourage women doctors and medical leaders with dedicated resources and flexible working arrangements that promote work-life balance…to shatter glass ceilings and glass fences”.
- The National Health Policy of 2017 clearly mentioned the Equity, Inclusiveness, and Decentralisation of decision making, alongwith local bodies and community participation in health policy-making to ensure more equitable and effective health outcomes.
- The policy also proposes a potentially achievable target of raising public health expenditure to 2.5% of the GDP in a time bound manner.
| Daily Main Question [Q] Analyse the impacts of centralisation of health policies in India. Do you think that a more decentralised approach would lead to more equitable health outcomes? |
Previous article
Role of Modern Technologies in India’s Affordable Housing
Next article
Changing the Growth Paradigm