
US Debt Ceiling Crisis
Syllabus: GS2/International Relations/GS3/Indian Economy
In News
The Democrats-led US government had in January hit its debt ceiling which could result into the government defaulting on its borrowings.
Structure of Government in USA
- The Federal Government is composed of three distinct branches: legislative, executive, and judicial, whose powers are vested by the U.S. Constitution in the Congress, the President, and the Federal courts, respectively.
What is the US debt ceiling?
- The debt ceiling, or debt limit, is the total amount the US government is allowed to borrow to finance its expenditure, such as paying salaries and welfare allowances.
- The debt limit was introduced in 1917, when the US entered World War I.
- Constitutionally, Congress controls the government’s expenditure. The debt ceiling was introduced in order to make it easier for the executive to operate without having to turn to Congress every time it wanted to spend — it allowed the government to borrow as required as long as it kept under the debt limit approved by Congress.
- Currently, this limit is at $31.4 trillion. The Republicans, who have a majority in the House, are refusing to raise it unless the Democrat-run government agrees to their demands, which include a significant cut in spending.
What happens if the govt defaults?
- The government would no longer have the money to function, and would have to decide who gets salaries, and how much.
- If Congress fails to increase the debt limit, it would cause severe hardship to American families, harm our global leadership position, and raise questions about our ability to defend our national security interests.
- Analysts say the dollar would weaken, the stock markets would collapse, and millions might lose their jobs. Also, the US’s credit rating would be downgraded, making future borrowing more expensive.
Measures adopted by US to Avert the Crisis :
President Joe Biden and Republican House Speaker Kevin McCarthy agreed on a deal that can potentially avert the crisis.
- A cap and a raise: Under the deal, the $31.4 trillion debt ceiling will be suspended until January 2025 — until after Biden’s current term. Until then, the government can keep borrowing to fund itself.
- In return, the White House has agreed to cap non-defence discretionary spending at 2023 levels in 2024, and increase it by 1% the year after.
- Work requirements made stricter: US president has agreed to increase work requirements for those who avail of government food stamps. The Supplemental Nutrition Assistance Program (SNAP) currently allows able-bodied people above 50 with no dependents to get the food stamps for three months “during any 36-month period when they cannot show they are employed or in a work or training program for at least 20 hours a week.
- Under the new deal, this age limit will be raised to 54. Veterans and the homeless are exempt from this.
- IRS, Covid fund: The Biden government had secured for beefing up the Internal Revenue System (IRS) sees a cut.
- The White House had argued that more staffers at the IRS would ensure the super-rich pay their taxes, boosting revenue. However, the Republicans had said this would lead to middle class Americans facing more tax hassle. Leftover Covid relief funds will be taken back, including that kept aside for tackling disasters.
- Streamlining energy projects approval: The government has agreed to the Republican demand of a more streamlined system of approval for energy projects.
Scenario In India
- According to Article 112 of the Indian Constitution, the annual financial statement of a year is a statement of the estimated receipts and expenditure of the government for that particular year((April 1st to March 31st).
- The term ‘Union Budget’ is nowhere mentioned in the Indian Constitution.
- The President of India is required to cause the annual financial statement to be laid before the Parliament.
- Article 266 of the Constitution requires the government to credit all revenues received by it, including taxes and other revenues, into the Consolidated Fund of India, unless otherwise provided by law.
- Article 266(2) of the Constitution requires the government to withdraw money from the Consolidated Fund of India only after it has been authorized by a law passed by the parliament. This ensures that the government cannot withdraw money from the Consolidated Fund without the approval of the parliament.
The Union Budget includes the following key components:
- Revenue Budget: This section details the government’s estimated revenue from various sources such as taxes, non-tax revenues and capital receipts. It shows how much money the government plans to earn from taxes, non-tax revenues, and other sources.
- Capital Budget: This section details the government’s proposed spending on various capital projects such as infrastructure development, capital investment in public sector enterprises, and other long-term investments. It shows how much money the government plans to spend on long-term projects like building new roads, bridges, and airports.
- Fiscal Deficit: The budget also includes an estimate of the fiscal deficit, which is the difference between the government’s total expenditure and its total revenue. The government aims to reduce the fiscal deficit to maintain financial stability.
- Tax Proposals: The budget also includes proposals for changes in tax laws and tax rates, which can have a significant impact on businesses and individuals.
Sources of Income for the Government
- Tax and Borrowings: Tax and borrowings are the major sources by which the government funds its expenditures. Besides this, the government also generates revenue from non-tax sources and via capital receipts.
- The Indian government’s main source of income is from Goods and Services Tax (GST) and income tax. Both forms constitute nearly 90% of the government’s total tax collection.
- Government’s business ventures: The non-tax resources are classified into three categories – currency, coinage and mint; interest receipts, dividends and profits and other non-tax receipts such as revenue from various government activities and services such as administrative services, public service commission, police, jails, agriculture and allied services.
- Disinvestment: A large portion of the capital receipts of the government is fuelled by revenue generated from disinvestments.
- To help raise the capital to meet its expenditures and to minimize the nation’s fiscal deficit, the government of India started the process of privatization of government establishments.
Source: IE
India’s Higher Education Sector
Syllabus: GS 2/Education
In News
Faculty shortages have existed in India’s higher education sector at least since the 1980s, but seem to have become permanent today.
India’s Higher Education
- The term ‘higher education’ with respect to India denotes the tertiary level education that is imparted after 12 years of schooling (10 years of primary education and 2 years of secondary education).
- The structure of Indian Higher Education is three-layered, consisting of Universities, Colleges, and Courses.
- All these institutions fall under the purview of the Ministry of Education.
Importance
- In today’s day and age, the premise that quality higher education is crucial for sustainable human development is undeniable.
- Higher education leads to acquiring analytical and problem-solving skills, ultimately helping humans to develop intellectual curiosity and character.
- It pushes the students to identify and set career goals that make them ready for professional setups.
- Therefore, a refined higher education enables economic, physical, and social well-being for a student.
Issues Linked
- It is crisis-ridden, understaffed, and underfunded.
- There is a huge shortage of teaching staff or faculty in the higher education system in India.
- Lack of reliable data on current faculty resources in colleges and universities.
- There is no standing mechanism to collect this information regularly.
- The government does collect data on colleges and universities, including the number of faculty members, for the annual All India Survey of Higher Education (AISHE), but this is a voluntary process for various institutions.
- The responsibility for the accuracy of the data rests with the concerned institution, meaning the information provided is not independently verified by any independent agency
- Most academic institutions have messy and incomplete websites containing only partial information about their faculty bodies.
- Different types of faculty shortages: There may even be an oversupply in some disciplines or locations and an acute shortage in others.
- Many private colleges and universities also hire less qualified people in poorly paid part-time positions instead of better qualified, regular faculty members, to keep costs down.
- Reservations reduce the pool of qualified people, sometimes severely.
- In Many cases, positions also remain vacant due to caste-based discrimination.
- Faculty positions remain vacant due to the unavailability of qualified applicants
- Unwillingness among faculty members to work at select institutions due to their unfavourable location .
- Other Issues: Indian universities persist in separating research and teaching activities, depriving students of exposure to cutting-edge ideas.
- Monetary incentives for academia are practically non-existent, and Indian R&D expenditure is one of the lowest in emerging economies.
- It is not surprising, then, that Indian universities rank low in both research and teaching
- Underrepresentation of some communities: Muslim community is lagging behind all communities, including the Scheduled Castes and Scheduled Tribes, in higher education(The AISHE Survey 2020-21)
- At a time when the enrolment of Scheduled Castes, Scheduled Tribes and Other Backward Classes (OBC) in higher education improved by 4.2%, 11.9% and 4%, respectively, compared with 2019-20, the Muslim community’s enrolment declined by 8%, numbering around 1,79,000 students.
- It is caused partially by the COVID-19 pandemic, points to the relative economic impoverishment of the community, which forces its talented students to pursue earning opportunities after completing schooling rather than enrolling for higher education, beginning at the graduation level.
Impacts
- India’s higher education system is structurally flawed and this crisis can affect innovation and human capital.
- Such flaws could affect macroeconomic indicators such as labour productivity, which is determined by innovation and human capital, among other things.
- The existing flows also undermines the growth of the country’s knowledge sector and hinder its aspiration to be recognised as a “Vishwa guru”.
Suggestions
- Colleges and universities need a sufficient number of teachers and researchers to create and disseminate knowledge.
- There is a need for a standing mechanism to monitor the size and quality of faculty resources and for data on faculty members to be made available on the website of every academic institution.
- In addition, an increase in research could lead to more innovation in the economy, which might in turn drive up labour productivity.
- Higher education has a potential twofold effect on productivity
- The government needs to ensure that higher education’s role in innovation and human capital is not ignored.
- The reforms must be pushed through and must lead to legislation that will fund research-based universities.
- this can bring a culture of discovery and accountability to India’s higher education institutions.
Source: TH
The violence faced by healthcare professionals
Syllabus: GS 2/Health
In News
- Recently a Dr. was stabbed to death in the line of duty in the Kollam district of Kerala.
About the Issue
- Over the years, there have been several episodes of physical and verbal violence.
- Each episode has the people at large passionately arguing the issue for a few days, only for their words to fade away until the next brutal incident.
- Doctors also stage protests but are ultimately honor-bound to return to duty, to reprise their roles as healers.
- Thus, the issue remains largely unaddressed.
|
Data Analysis
|
Causes
- Often, patients or their relatives turn to violence because the healthcare system hasn’t met their expectations.
- Some perpetrators become violent over concerns about the patient’s condition, such as actual or perceived deterioration of their condition or doubts about the wrong treatment being administered.
- Some others become violent due to issues such as high payment dues and protracted waiting times.
Effect of Violence
- Psychological Impact: Being on the receiving end of verbal or physical violence has an immense psychological impact.
- Some studies have reported symptoms of post-traumatic stress disorder, anxiety, and depression in doctors who have faced violence from patients or their kin.
- Effect Rural Healthcare: India has a skewed doctor-patient ratio (1:854, including Ayurveda and homeopathy practitioners), doctors often decide to operate in resource-abundant settings for their own security. This in turn affects rural healthcare.
- Effect Quality of Healthcare: After experiencing violence, the PLoS ONE study found that doctors wish to stop offering emergency services, refer patients sooner to more specialists, and over-investigate symptoms and prescribe more tests.
- They also tend to offer less lifesaving medical and surgical interventions that a patient may require, over fear that a risky procedure may provoke violent action. This negatively affects the quality of healthcare.
|
How China handled this type of Challenge and Lessons for India
|
Suggestions
- We must spend more money to strengthen the system from the grassroots level, such as reducing long waiting periods for treatment.
- The availability and accessibility of medicines, tests, and financial aid for those in need will greatly reduce their stress, instead of leaving them to hold their physicians responsible for it.
- Healthcare professionals need to work on their communication skills and ensure meticulous documentation.
- At the same time, measures to mitigate workplace violence towards them must be multi-pronged and focus on institutional and policy measures.
- Ensuring that there are counselors to help patients and relatives in times of high emotional distress (together with people who can translate between languages) can eliminate any miscommunication regarding a patient’s condition and treatment.
- In addition, a robust security system and not allowing more than a few relatives by a patient’s bedside may also be important — as well as enforcing the law well enough to bring perpetrators to book in a reasonable span of time.
- There is a need to learn from China that such policies in India would improve Indians’ trust in the Indian healthcare system as well.
Source: TH
Hysterectomies
Syllabus :GS 2/Health
In News
The Union Health Ministry recently urged State governments to audit hysterectomy trends in public and private hospitals, in response to a Supreme Court petition arguing that women from marginalised locations are at risk of unjustified hysterectomies for economic gains and exploitation.
- The Court also gave a three-month deadline to States, directing them to implement the guidelines previously issued by the Centre.
About Hysterectomy
- Hysterectomy is an operation to remove the uterus.
- the criteria for getting a hysterectomy: The highest percentage of hysterectomies were to treat excessive menstrual bleeding or pain (51.8%); 24.94% for fibroids; 24.94% for cysts and 11.08% for uterine disorder or rupture, according to NFHS-5 data. Yet, studies have shown that “many of these causes were considered to be treatable and surgery could be avoided”.
- A majority of these cases were reported among socially and economically disadvantaged women.
Existing Issues
- The procedure can easily be misused by either private clinics who earn profits (from insurance money) or by contractors in unorganised sectors such as the sugar-cane-cutting industry, where ‘wombless women’ are the norm to eliminate the need for menstrual care and hygiene among workers.
- despite the provisions, private hospitals in Bihar, Chhattisgarh and Rajasthan engaged in unethical practices, unnecessary procedures and did not inform women of side effects or take their informed consent.
- In doing so, they “failed in providing and regulating constitutionally mandated reproductive healthcare to women” and violated their “rights to health, bodily integrity and informed consent
Effect
- Hysterectomies may cause long-term injuries and disabilities, requiring follow-up and post-operative care, both rarely available or affordable.
- In some cases, where hysterectomies are not justified yet still done, women may continue to suffer post-surgery and might need additional surgery.
Governments Step
- The Union Health Ministry in 2022 issued guidelines to prevent unnecessary hysterectomies — listing possible indications of when hysterectomy may be required and alternative clinical treatments for gynaecological issues.
- Further, they recommended setting up district, State-level and national hysterectomy monitoring committees to monitor and collect data on age, mortality, and occupations, among other details.
- The monitoring committees are also tasked with creating awareness, among both practitioners and patients, about bodily anatomy, the role of uterus and when hysterectomies are actually indicated.
- The government’s flagship health insurance programme, the Ayushman Bharat Pradhan Mantri Jan Arogya Yojana provides health cover of ₹5 lakh for 1,949 procedures, including hysterectomies.
- The government has authorised 45,434 hospitals to conduct these operations.
Source: TH
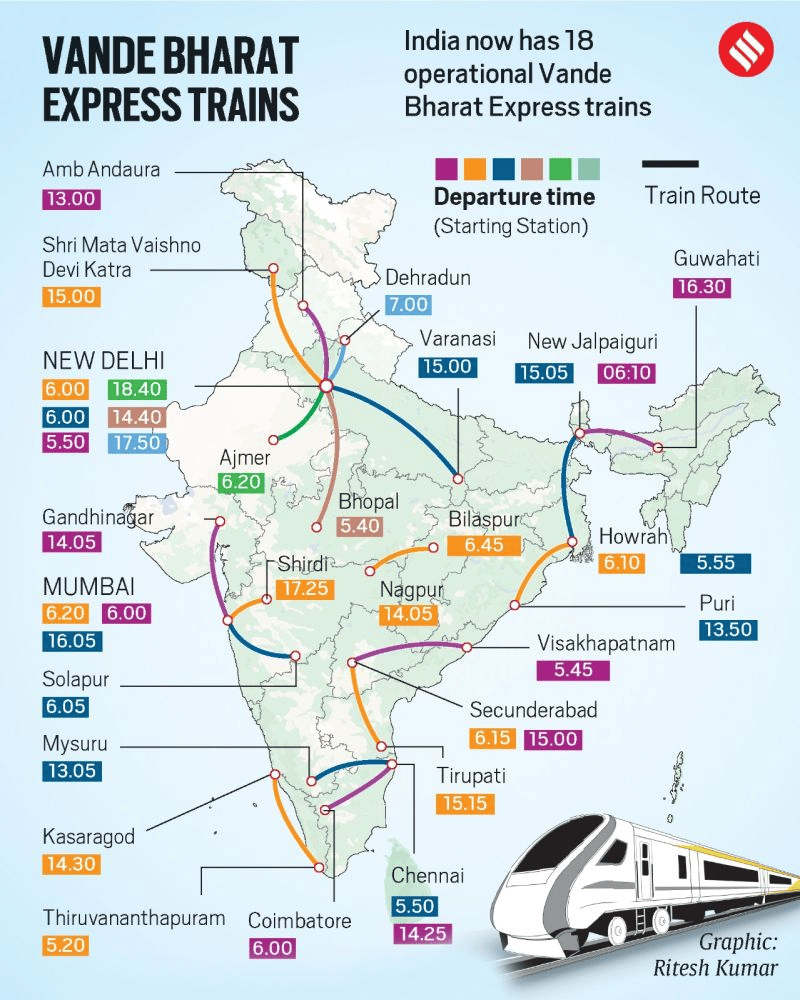
VANDE BHARAT EXPRESS
GS-3/Economy
News:
· Prime Minister Narendra Modi flagged off Assam’s first Vande Bharat Express. The Vande Bharat Express will connect Guwahati with New Jalpaiguri.
About
· The Vande Bharat Express was formerly known as Train 18.
· It is an electric multiple-unit train operated by Indian Railways.
· It can reach operating speed to 160 km/h.
· The train is designed by the Research Designs & Standards Organisation (RDSO), Lucknow and manufactured by the Integral Coach Factory (ICF), Chennai.
· The first Vande Bharat train was flagged off on the New Delhi- Kanpur- Allahabad-Varanasi route in 2019.
DISEASE X
GS-3/Science and Tech
News
· After announcing that that COVID-19 was no longer a global health emergency, the World Health Organization (WHO) warned that “Disease X” can lead to an “even deadlier” pandemic.
Disease X
· Disease X is not real yet and has not been identified in any human beings.
· It represent a hypothetical, unknown pathogen that could cause a future epidemic.
· The name was adopted by the WHO in 2018 on their shortlist of blueprint priority diseases to ensure that their planning was sufficiently flexible to adapt to an unknown pathogen.
· Disease X could also be zoonotic meaning that it could be caused by germs jumping from animals to humans
Priority List
· Apart from Disease X, Covid-19, Crimean-Congo haemorrhagic fever, Ebola virus disease, Marburg virus disease, Lassa fever, MERS-CoV and SARS, Nipah and henipaviral diseases, Rift Valley fever and Zika are other diseases on WHO’s priority diseases list.